Intermittent Diplopia in the Elderley
Case Study: Intermittent Diplopia in the Elderly
Dr Elaine Wong
Presentation
80 yo female presented with intermittent diplopia over the last 6-12 months. On further questioning, the diplopia is horizontal in nature and is only present when she is sitting in the car as a passenger (she is no longer driving). She does not get any diplopia when reading or watching TV. There is no history of fatiguability or fluctuation of eyelid position. She does not experience any headaches or other neurological symptoms. She has a history of diabetes and hypertension.
Clinical findings
- VAR s 6/9 VAL s 6/9
- Anterior : Bilateral psuedophakia
- Fundus: No signs of diabetic/ hypertensive retinopathy, glaucoma or macular degeneration
- Ocular motility: Esotropia of 4 dioptres in primary position but worse in right, left and downgaze. Reduced elevation in both eyes
//
ET 12^
ET 4^
ET 10^
ET 8^
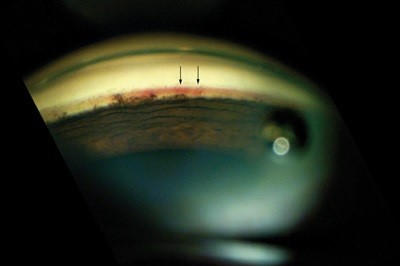
- External examinations:
What do you see?
Bilateral ptosis, high lid crease and deep superior sulcus.
What investigation would you perform next?
MRI brain and orbit.
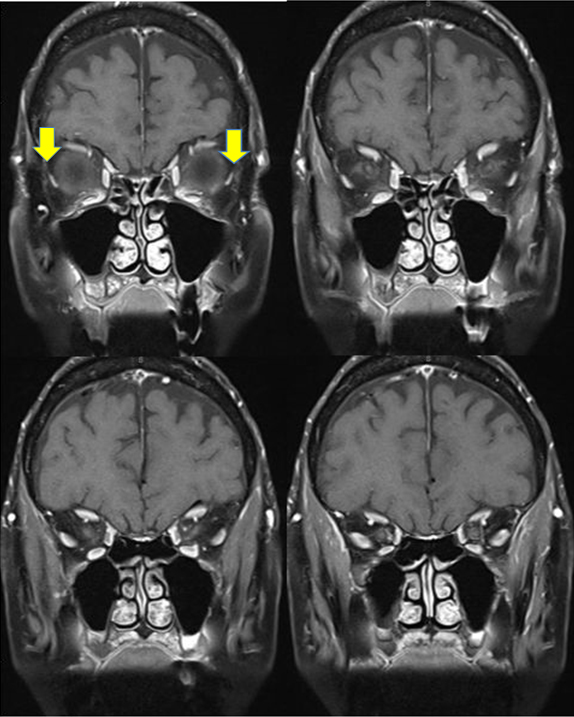
What do you see?
There is downward displacement of the lateral recti.
What is the diagnosis?
Sagging eye syndrome
Discussion
Sagging eye syndrome (SES) is a newly recognised condition first described by Rutar and Demer in 2009. It is strabismus caused by involutional changes in the intermuscular connective tissue septum between superior rectus and lateral rectus. This produce an inferomedial displacement of the lateral rectus muscle belly. Mechanically, this positional change of lateral rectus results in weakening of its abducting ability and give it an infraduction and excyclotorsion action. This leads to esotropia, hypotropia or divergence insufficiency pattern of strabismus. It is a mechanical cause of acquired, small angle horizontal or vertical strabismus in the elderly population.
Typically, patients present with sub-acute onset of diplopia which can be vertical or horizontal in nature. It is often accompanied by aponeurotic ptosis, high lid crease and deep superior sulci due to age-related degeneration of levator tendon and disinsertion from the superior tarsal plate.
Management
As strabismus due to SES is often small angle, prism glasses are often adequate in addressing the issues. Surgery will be reserve for severe cases and will be aimed to restore normal extraocular muscle anatomy.
{kind=link}